A. How do we evaluate visual disorders?
1. What are visual disorders? Visual disorders
are abnormalities of the eye, the optic nerve, the optic tracts, or the brain that may cause a loss of visual acuity or visual
fields. A loss of visual acuity limits your ability to distinguish detail, read, or do fine work. A loss of visual
fields limits your ability to perceive visual stimuli in the peripheral extent of vision.
2. How do we define
statutory blindness? Statutory blindness is blindness as defined in sections 216(i)(1) and 1614(a)(2) of the Social
Security Act (the Act). The Act defines blindness as visual acuity of 20/200 or less in the better eye with the use
of a correcting lens. We use your best-corrected visual acuity for distance in the better eye when we determine if this
definition is met. The Act also provides that an eye that has a visual field limitation such that the widest diameter
of the visual field subtends an angle no greater than 20 degrees is considered as having visual acuity of 20/200 or less.
You have statutory blindness only if your visual disorder meets the criteria of 2.02 or 2.03A. You do not have statutory
blindness if your visual disorder medically equals the criteria of 2.02 or 2.03A, or if it meets or medically equals 2.03B,
2.03C, or 2.04. If your visual disorder medically equals the criteria of 2.02 or 2.03A, or if it meets or medically
equals 2.03B, 2.03C, or 2.04, we will find that you have a disability if your visual disorder also meets the duration requirement.
3. What evidence do we need to establish statutory blindness under title XVI? For title XVI, the only evidence
we need to establish statutory blindness is evidence showing that your visual acuity in your better eye or your visual field
in your better eye meets the criteria in 2.00A2, provided that those measurements are consistent with the other evidence in
your case record. We do not need to document the cause of your blindness. Also, there is no duration requirement
for statutory blindness under title XVI (see §§416.981 and 416.983).
4. What evidence do we need
to evaluate visual disorders, including those that result in statutory blindness under title II?
a. To evaluate
your visual disorder, we usually need a report of an eye examination that includes measurements of the best-corrected visual
acuity or the extent of the visual fields, as appropriate. If there is a loss of visual acuity or visual fields, the
cause of the loss must be documented. A standard eye examination will usually reveal the cause of any visual acuity
loss. An eye examination can also reveal the cause of some types of visual field deficits. If the eye examination
does not reveal the cause of the visual loss, we will request the information that was used to establish the presence of the
visual disorder.
b. A cortical visual disorder is a disturbance of the posterior visual pathways or occipital lobes of
the brain in which the visual system does not interpret what the eyes are seeing. It may result from such causes as
traumatic brain injury, stroke, cardiac arrest, near drowning, a central nervous system infection such as meningitis or encephalitis,
a tumor, or surgery. It can be temporary or permanent, and the amount of visual loss can vary. It is possible
to have a cortical visual disorder and not have any abnormalities observed in a standard eye examination. Therefore,
a diagnosis of a cortical visual disorder must be confirmed by documentation of the cause of the brain lesion. If neuroimaging
or visual evoked response (VER) testing was performed, we will request a copy of the report or other medical evidence that
describes the findings in the report.
c. If your visual disorder does not satisfy the criteria in 2.02, 2.03, or 2.04,
we will also request a description of how your visual disorder impacts your ability to function.
5. How
do we measure best-corrected visual acuity?
a. Testing for visual acuity. When we need to measure your
best-corrected visual acuity, we will use visual acuity testing that was carried out using Snellen methodology or any other
testing methodology that is comparable to Snellen methodology.
b. Determining best-corrected visual acuity.
(i) Best-corrected visual acuity is the optimal visual acuity attainable with the use of a corrective lens. In
some instances, this assessment may be performed using a specialized lens; for example, a contact lens. We will use
the visual acuity measurements obtained with a specialized lens only if you have demonstrated the ability to use the specialized
lens on a sustained basis. However, we will not use visual acuity measurements obtained with telescopic lenses because
they significantly reduce the visual field. If you have an absent response to VER testing in an eye, we can determine
that your best-corrected visual acuity is 20/200 or less in that eye. However, if you have a positive response to VER
testing in an eye, we will not use that result to determine your best-corrected visual acuity in that eye. Additionally,
we will not use the results of pinhole testing or automated refraction acuity to determine your best-corrected visual acuity.
(ii) We will use the best-corrected visual acuity for distance in your better eye when we determine whether your loss of
visual acuity satisfies the criteria in 2.02. The best-corrected visual acuity for distance is usually measured by determining
what you can see from 20 feet. If your visual acuity is measured for a distance other than 20 feet, we will convert
it to a 20-foot measurement. For example, if your visual acuity is measured at 10 feet and is reported as 10/40, we
will convert this to 20/80.
6. How do we measure visual fields?
a. Testing for visual
fields.
(i) We generally need visual field testing when you have a visual disorder that could result in visual field
loss, such as glaucoma, retinitis pigmentosa, or optic neuropathy, or when you display behaviors that suggest a visual field
loss.
(ii) When we need to measure the extent of your visual field loss, we will use visual field measurements
obtained with an automated static threshold perimetry test performed on a perimeter, like the Humphrey Field Analyzer, that
satisfies all of the following requirements:
A. The perimeter must use optical projection to generate the test stimuli.
B. The perimeter must have an internal normative database for automatically comparing your performance with that of
the general population.
C. The perimeter must have a statistical analysis package that is able to calculate visual
field indices, particularly mean deviation.
D. The perimeter must demonstrate the ability to correctly detect visual
field loss and correctly identify normal visual fields.
E. The perimeter must demonstrate good test-retest reliability.
F. The perimeter must have undergone clinical validation studies by three or more independent laboratories with results
published in peer-reviewed ophthalmic journals.
(iii) The test must use a white size III Goldmann stimulus and a 31.5
apostilb (10 cd/m2) white background. The stimuli locations must be no more than 6 degrees apart horizontally or vertically.
Measurements must be reported on standard charts and include a description of the size and intensity of the test stimulus.
(iv) To determine statutory blindness based on visual field loss (2.03A), we need a test that measures the central
24 to 30 degrees of the visual field; that is, the area measuring 24 to 30 degrees from the point of fixation. Acceptable
tests include the Humphrey 30-2 or 24-2 tests.
(v) The criterion in 2.03B is based on the use of a test performed on
a Humphrey Field Analyzer that measures the central 30 degrees of the visual field. We can also use comparable results
from other acceptable perimeters, for example, a mean defect of 22 on an acceptable Octopus test, to determine that the criterion
in 2.03B is met. We cannot use tests that do not measure the central 30 degrees of the visual field, such as the Humphrey
24-2 test, to determine if your impairment meets or medically equals 2.03B.
(vi) We measure the extent of visual field
loss by determining the portion of the visual field in which you can see a white III4e stimulus. The “III” refers
to the standard Goldmann test stimulus size III, and the “4e” refers to the standard Goldmann intensity filters
used to determine the intensity of the stimulus.
(vii) In automated static threshold perimetry, the intensity of the
stimulus varies. The intensity of the stimulus is expressed in decibels (dB). We need to determine the dB level
that corresponds to a 4e intensity for the particular perimeter being used. We will then use the dB printout to determine
which points would be seen at a 4e intensity level. For example, in Humphrey Field Analyzers, a 10 dB stimulus is equivalent
to a 4e stimulus. A dB level that is higher than 10 represents a dimmer stimulus, while a dB level that is lower than
10 represents a brighter stimulus. Therefore, for tests performed on Humphrey Field Analyzers, any point seen at 10
dB or higher is a point that would be seen with a 4e stimulus.
(viii) We can also use visual field measurements
obtained using kinetic perimetry, such as the Humphrey “SSA Test Kinetic” or Goldmann perimetry, instead of automated
static threshold perimetry. The kinetic test must use a white III4e stimulus projected on a white 31.5 apostilb (10
cd/m2) background. In automated kinetic tests, such as the Humphrey “SSA Test Kinetic,” testing along a
meridian stops when you see the stimulus. Because of this, automated kinetic testing does not detect limitations in
the central visual field. If your visual disorder has progressed to the point at which it is likely to result in a significant
limitation in the central visual field, such as a scotoma (see 2.00A8c), we will not use automated kinetic perimetry to evaluate
your visual field loss. Instead, we will assess your visual field loss using automated static threshold perimetry or
manual kinetic perimetry.
(ix) We will not use the results of visual field screening tests, such as confrontation tests,
tangent screen tests, or automated static screening tests, to determine that your impairment meets or medically equals a listing
or to evaluate your residual functional capacity. However, we can consider normal results from visual field screening
tests to determine whether your visual disorder is severe when these test results are consistent with the other evidence in
your case record. (See §§404.1520(c), 404.1521, 416.920(c), and 416.921.) We will not consider normal test
results to be consistent with the other evidence if either of the following applies:
A. The clinical findings indicate
that your visual disorder has progressed to the point that it is likely to cause visual field loss, or
B. You have
a history of an operative procedure for retinal detachment.
b. Use of corrective lenses. You must not wear eyeglasses
during the visual field examination because they limit your field of vision. Contact lenses or perimetric lenses may
be used to correct visual acuity during the visual field examination in order to obtain the most accurate visual field measurements.
For this single purpose, you do not need to demonstrate that you have the ability to use the contact or perimetric lenses
on a sustained basis.
7.How do we calculate visual efficiency?
a. Visual acuity efficiency.
We use the percentage shown in Table 1 that corresponds to the best-corrected visual acuity for distance in your better eye.
b. Visual field efficiency. We use kinetic perimetry to calculate visual field efficiency by adding the number of degrees
seen along the eight principal meridians in your better eye and dividing by 500. (See Table 2.)
c. Visual efficiency.
We calculate the percent of visual efficiency by multiplying the visual acuity efficiency by the visual field efficiency and
converting the decimal to a percentage. For example, if your visual acuity efficiency is 75 percent and your visual
field efficiency is 64 percent, we will multiply 0.75 x 0.64 to determine that your visual efficiency is 0.48, or 48 percent.
8. How do we evaluate specific visual problems?
a. Statutory blindness. Most test charts that use
Snellen methodology do not have lines that measure visual acuity between 20/100 and 20/200. Newer test charts, such
as the Bailey-Lovie or the Early Treatment Diabetic Retinopathy Study (ETDRS), do have lines that measure visual acuity between
20/100 and 20/200. If your visual acuity is measured with one of these newer charts, and you cannot read any of the
letters on the 20/100 line, we will determine that you have statutory blindness based on a visual acuity of 20/200 or less.
For example, if your best-corrected visual acuity for distance in the better eye was determined to be 20/160 using an ETDRS
chart, we will find that you have statutory blindness. Regardless of the type of test chart used, you do not have statutory
blindness if you can read at least one letter on the 20/100 line. For example, if your best-corrected visual acuity
for distance in the better eye was determined to be 20/125+1 using an ETDRS chart, we will find that you do not have statutory
blindness as you are able to read one letter on the 20/100 line.
b. Blepharospasm. This movement disorder is characterized
by repetitive, bilateral, involuntary closure of the eyelids. If you have this disorder, you may have measurable visual
acuities and visual fields that do not satisfy the criteria of 2.02 or 2.03. Blepharospasm generally responds to therapy.
However, if therapy is not effective, we will consider how the involuntary closure of your eyelids affects your ability to
maintain visual functioning over time.
c. Scotoma. A scotoma is a non-seeing area in the visual field surrounded
by a seeing area. When we measure the visual field, we subtract the length of any scotoma, other than the normal blind spot,
from the overall length of any diameter on which it falls.
B.How do we evaluate hearing loss?
1.What
evidence do we need?
a. We need evidence showing that you have a medically determinable impairment that
causes your hearing loss and audiometric measurements of the severity of your hearing loss. We generally require both a complete
otologic examination and audiometric testing to establish that you have a medically determinable impairment that causes your
hearing loss. You should have this audiometric testing within 2 months of the complete otologic examination. Once we have
evidence that you have a medically determinable impairment, we can use the results of later audiometric testing to assess
the severity of your hearing loss without another complete otologic examination. We will consider your test scores together
with any other relevant information we have about your hearing, including information from outside of the test setting.
b.
The complete otologic examination must be performed by a licensed physician (medical or osteopathic doctor). It must include
your medical history, your description of how your hearing loss affects you, and the physician's description of the appearance
of the external ears (pinnae and external ear canals), evaluation of the tympanic membranes, and assessment of any middle
ear abnormalities.
c. Audiometric testing must be performed by, or under the direct supervision of, an otolaryngologist
or by an audiologist qualified to perform such tests. We consider an audiologist to be qualified if he or she is currently
and fully licensed or registered as a clinical audiologist by the State or U.S. territory in which he or she practices. If
no licensure or registration is available, the audiologist must be currently certified by the American Board of Audiology
or have a Certificate of Clinical Competence (CCC-A) from the American Speech-Language-Hearing Association (ASHA).
2.
What audiometric testing do we need when you do not have a cochlear implant?
a. We generally need pure
tone air conduction and bone conduction testing, speech reception threshold (SRT) testing (also referred to as "spondee
threshold'' or "ST"' testing), and word recognition testing (also referred to as "word discrimination'' or
``speech discrimination'' testing). This testing must be conducted in a sound-treated booth or room and must be in accordance
with the most recently published standards of the American National Standards Institute (ANSI). Each ear must be tested separately.
b. You must not wear hearing aids during the testing. Additionally, a person described in 2.00B1c must perform an otoscopic
examination immediately before the audiometric testing. (An otoscopic examination provides a description of the appearance
of your external ear canals and an evaluation of the tympanic membranes. In these rules, we use the term to include otoscopic
examinations performed by physicians and otoscopic inspections performed by audiologists and others.) The otoscopic examination
must show that there are no conditions that would prevent valid audiometric testing, such as fluid in the ear, ear infection,
or obstruction in an ear canal. The person performing the test should also report on any other factors, such as your cooperation
with the test, that can affect the interpretation of the test results.
c. To determine whether your hearing loss meets
the air and bone conduction criteria in 2.10A, we will average your air and bone conduction hearing thresholds at 500, 1000,
and 2000 Hertz (Hz). If you do not have a response at a particular frequency, we will use a threshold of 5 decibels (dB) over
the limit of the audiometer.
d. The SRT is the minimum dB level required for you to recognize 50 percent of the words
on a standard list of spondee words. (Spondee words are two-syllable words that have equal stress on each syllable.) The SRT
is usually within 10 dB of the average pure tone air conduction hearing thresholds at 500, 1000, and 2000 Hz. If the SRT is
not within 10 dB of the average pure tone air conduction threshold, the reason for the discrepancy must be documented. If
we cannot determine that there is a medical basis for the discrepancy, we will not use the results of the testing to determine
whether your hearing loss meets a listing.
e. Word recognition testing determines your ability to recognize a standardized
list of phonetically balanced monosyllabic words in the absence of any visual cues. This testing must be performed in quiet.
The list may be recorded or presented live, but in either case the words should be presented at a level of amplification that
will measure your maximum ability to discriminate words, usually 35 to 40 dB above your SRT. However, the amplification level
used in the testing must be medically appropriate, and you must be able to tolerate it. If you cannot be tested at 35 to 40
dB above your SRT, the person who performs the test should report your word recognition testing score at your highest comfortable
level of amplification.
3.What audiometric testing do we need when you have a cochlear implant?
a. If you have a cochlear implant, we will consider you to be disabled until 1 year after initial implantation.
b.
After that period, we need word recognition testing performed with any version of the Hearing in Noise Test (HINT) to determine
whether your impairment meets 2.11B. This testing must be conducted in quiet in a sound field. Your implant must be functioning
properly and adjusted to your normal settings. The sentences should be presented at 60 dB HL (Hearing Level) and without any
visual cues.
4.How do we evaluate your word recognition ability if you are not fluent in English?
If
you are not fluent in English, you should have word recognition testing using an appropriate word list for the language in
which you are most fluent. The person conducting the test should be fluent in the language used for the test. If there is
no appropriate word list or no person who is fluent in the language and qualified to perform the test, it may not be possible
to measure your word recognition ability. If your word recognition ability cannot be measured, your hearing loss cannot meet
2.10B or 2.11B. Instead, we will consider the facts of your case to determine whether you have difficulty understanding words
in the language in which you are most fluent, and if so, whether that degree of difficulty medically equals 2.10B or 2.11B.
For example, we will consider how you interact with family members, interpreters, and other persons who speak the language
in which you are most fluent.
C. How do we evaluate vertigo associated with disturbances of labyrinthine-vestibular
function, including Ménière's disease?
1. Vertigo associated with disturbances of labyrinthine-vestibular
function, including Ménière's disease. These disturbances of balance are characterized by a hallucination
of motion or a loss of position sense and a sensation of dizziness which may be constant or may occur in paroxysmal attacks.
Nausea, vomiting, ataxia, and incapacitation are frequently observed, particularly during the acute attack. It is important
to differentiate the report of rotary vertigo from that of "dizziness" which is described as light-headedness, unsteadiness,
confusion, or syncope.
2. Ménière's disease is characterized by paroxysmal attacks of
vertigo, tinnitus, and fluctuating hearing loss. Remissions are unpredictable and irregular, but may be long-lasting;
hence, the severity of impairment is best determined after prolonged observation and serial reexaminations.
3.
The diagnosis of a vestibular disorder requires a comprehensive neuro-otolaryngologic examination with a detailed description
of the vertiginous episodes, including notation of frequency, severity, and duration of the attacks. Pure tone and speech
audiometry with the appropriate special examinations, such as Bekesy audiometry, are necessary. Vestibular function
is accessed by positional and caloric testing, preferably by electronystagmography. When polytomograms, contrast radiography,
or other special tests have been performed, copies of the reports of these tests should be obtained in addition to appropriate
medically acceptable imaging reports of the skull and temporal bone. Medically acceptable imaging includes, but is not
limited to, x-ray imaging, computerized axial tomography (CAT scan) or magnetic resonance imaging (MRI), with or without contrast
material, myelography, and radiocnuclear bone scans. “Appropriate” means that the technique used is the
proper one to support the evaluation and diagnosis of the impairment. .
D. Loss of speech.
In
evaluating the loss of speech, the ability to produce speech by any means includes the use of mechanical or electronic devices
that improve voice or articulation. Impairments of speech may also be evaluated under the body system for the underlying
disorder, such as neurological disorders, 11.00ff.
E. How do we evaluate impairments that do not meet one of
the special senses and speech listings?
1. These listings are only examples of common special senses
and speech disorders that we consider severe enough to prevent an individual from doing any gainful activity. If your
impairment(s) does not meet the criteria of any of these listings, we must also consider whether you have an impairment(s)
that satisfies the criteria of a listing in another body system.
2. If you have a medically determinable impairment(s)
that does not meet a listing, we will determine whether the impairment(s) medically equals a listing. (See §§404.1526
and 416.926.) If you have an impairment(s) that does not meet or medically equal a listing, you may or may not have
the residual functional capacity to engage in substantial gainful activity. Therefore, we proceed to the fourth, and
if necessary, the fifth steps of the sequential evaluation process in §§404.1520 and 416.920. When we decide
whether you continue to be disabled, we use the rules in §§404.1594, 416.994, or 416.994a, as appropriate.
2.01
Category of Impairments, Special Senses and Speech
2.02 Loss of Visual Acuity.
Remaining vision in the better eye after best correction is 20/200 or less.
2.03 Contraction
of the visual field in the better eye, with:
A . The widest diameter subtending an angle around
the point of fixation no greater than 20 degrees;
OR
B. A mean deviation of –22 or worse, determined
by automated static threshold perimetry as described in 2.00A6a (v);
OR
C. A visual field efficiency of
20 percent or less as determined by kinetic perimetry (see 2.00A7b).
2.04 Loss of visual
efficiency. Visual efficiency of the better eye of 20 percent or less after best correction (see 2.00A7c).
2.07
Disturbance of labyrinthine-vestibular function (Including Ménière's disease), characterized by
a history of frequent attacks of balance disturbance, tinnitus, and progressive loss of hearing. With both A and B:
A. Disturbed function of vestibular labyrinth demonstrated by caloric or other vestibular tests; and
B.
Hearing loss established by audiometry.
2.09 Loss of speech due to any
cause, with inability to produce by any means speech that can be heard, understood, or sustained.
2.10
Hearing loss not treated with cochlear implantation.
A. An average air conduction hearing threshold
of 90 decibels or greater in the better ear and an average bone conduction hearing threshold of 60 decibels or greater in
the better ear (see 2.00B2c).
OR
B. A word recognition score of 40 percent or less in the better ear determined
using a standardized list of phonetically balanced monosyllabic words (see 2.00B2e).
2.11
Hearing loss treated with cochlear implantation.
A. Consider under a disability for 1 year after
initial implantation.
OR
B. If more than 1 year after initial implantation, a word recognition score of
60 percent or less determined using the HINT (see 2.00B3b).
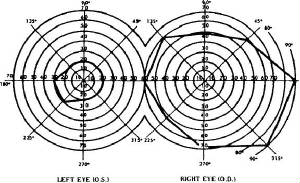
1. The diagram of the right eye illustrates the extent of a normal visual field as measured with a III4e stimulus. The
sum of the eight principal meridians of this field is 500 degrees.
2. The diagram of the left eye illustrates a visual
field contracted to 30 degrees in two meridians and to 20 degrees in the remaining six meridians. The percent of visual field
efficiency of this field is: (2 × 30) + (6 × 20) = 180÷500 = 0.36 or 36 percent visual field efficiency.